How will Medicaid cuts affect disability services?
Medicaid provides crucial healthcare and disability services to millions across the country, but this funding is in jeopardy after congress passed large medicaid cuts under the One Big Beautiful Bill Act. Funding cuts, stricter eligibility rules, and reduced home and community based services are forcing families to seek affordable alternatives. These changes disproportionately impact seniors, people with disabilities, and low-income households, making it even harder to access essential care without facing financial strain. Today we’ll explore how Medicaid cuts are affecting support systems and how cost-effective solutions, like GrandCare, can help bridge the gap.
Medicaid provides coverage to over 85 million Americans, including 10 million people with disabilities, who rely on it for home and community-based services (HCBS). According to the Berkeley School of Public Health, the One Big Beautiful Bill Act will cut medicaid spending by over 15% across the country (Dow, 2025). These cuts will come in forms of stricter eligibility requirements, higher out-of-pocket costs, and longer wait times for waiver programs While the true effects of these cuts are still uncertain, many who rely on medicaid for disability services have ample cause for concern.
“Medicaid is more than low-income health insurance. It is frequently the only option for Utahns who need intensive mental health care or long-term services and supports not usually available in the private market.” (Disability Law Center, 2025)
Currently, adults with I/DD are lacking a large amount of independence in their living situations and daily lives. 72% of these adults are living at home with a caregiver (Braddock, 2013) This sinks time and money into hands-on caregivers when many adults could be using GrandCare touchscreen and remote supports technology to be self-supporting in their own homes with more independence and less oversight. These costly services could become increasingly unaffordable as the weight of the medicaid cuts are starting to be felt. An in house aide costs around $7,000 monthly on average, while an assisted living facility costs over $5,000 monthly (UltimateCare, 2025).
How Can GrandCare Bridge the Gap?
Technology is reshaping how we approach care by creating new opportunities for efficiency and independence. GrandCare Systems, the leader in the smart home industry, is making strides by automating daily support, producing innovative systems that reduce in-home staff, increasing independence for adults with I/DD, all while still maintaining quality care.
Firstly, GrandCare has been shown to greatly reduce the required support staff needed to provide adequate care. By being able to automate many of the menial tasks such as taking medications and todo lists, staffing costs can be greatly reduced. A study by Xavier University found that smart home technology, like GrandCare, cut caregiver related expenses by nearly half (Denault, 2021). By automating reminders, monitoring daily activities, and alerting caregivers only when necessary, the system reduces unnecessary in-person check-ins which lowers labor costs. This efficiency allows healthcare providers to give high-quality care with a limited budget. With fewer caregiver hours required, families and healthcare systems alike can allocate resources more effectively, making GrandCare a smart investment for sustainable, long-term care solutions.
Additionally, Grandcare can help reduce unnecessary healthcare spending by improving medication adherence. Medication adherence is defined as the extent to which a person’s behavior such as taking medications, following diets, or changing their lifestyle aligns with their doctor’s recommendations. A lack of medication adherence is a major source of waste in the healthcare industry. Studies show that over 25% of hospitalizations stem from patients not taking medications as prescribed, costing the healthcare system between $100 and $300 billion annually (Kim, 2018). By implementing solutions like the GrandCare System, which reminds users to take their medications and alerts caregivers if doses are missed, we can significantly reduce avoidable hospital visits and the costs associated with it. This proactive approach not only enhances patient outcomes but also helps preserve limited funding by cutting wasteful and unnecessary spending. Investing in GrandCare ensures that limited resources are used efficiently, benefiting both patients and the healthcare system as a whole.
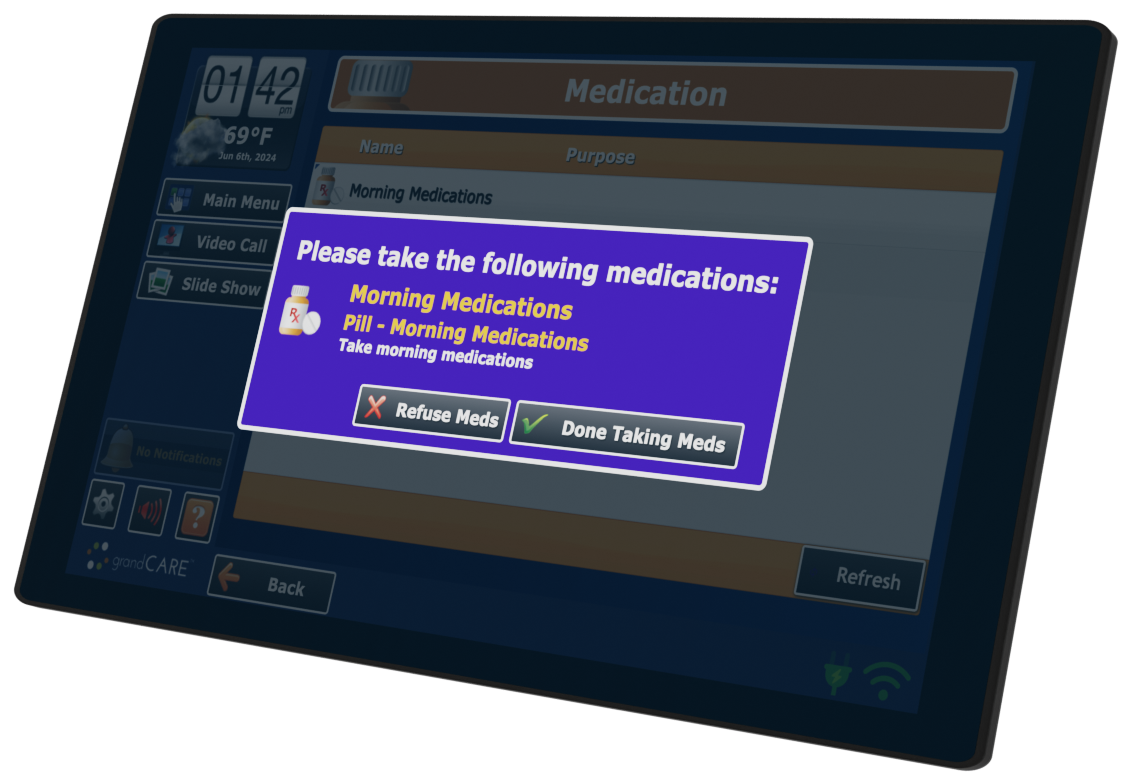
For adults with I/DD, many struggle with very limited independence. Many adults with I/DD have the potential to live life more independently, they just need the right tools to succeed. Research confirms that the only skills required for independence are mastering safety awareness, self-care, and medication management (Dimitriadou, 2018). With GrandCare’s innovative support system, individuals with I/DD gain the tools to take control of their daily lives. The system provides reminders for medications, prompts for personal care tasks, and instant safety notifications, all while keeping caregivers connected only when needed. This balance of independence and support empowers users to build confidence, reduce reliance on others, and experience more independence. It allows for an increased sense of autonomy while still giving caregivers and family peace of mind.
One striking example of this involves an Ohio man who, in spite of being fairly independent, required an awake support staff in his home every night. This was because he has a sleep-related eating disorder which meant that he would sometimes get up in the middle of the night, sleepwalk into his kitchen and once there eat everything he could get his hands on. It was such a concern for his wellbeing that he required a staff member to be present for the entire overnight shift. The staff person’s only intervention was to approach the man and suggest that he go back to bed.
But now that he has GrandCare technology there is a motion sensor in his kitchen that alerts remote support staff if it sees activity there in the overnight hours. That remote support person can video call directly into the man’s kitchen and suggest that he should probably go back to bed. GrandCare views this as “just in time” support as opposed to “just in case” support. The man now has the dignity and privacy of being alone in his home every night while still getting exactly the right support at exactly the right time. Instead of eight hours of in-person support, he now has sixty seconds of remote support, which is all he really needs.
Another example concerns a man with I/DD who required two hours of in-person support every day to help him navigate his morning routine. But now that he has GrandCare he uses technology to remind himself to do all the tasks that add up to a successful morning. He no longer has in-person support for this.
Conclusion
While upcoming Medicaid cuts and funding uncertainties create concerns for care providers, agencies have an opportunity to take proactive steps today that safeguard both their clients’ wellbeing as well as their organization’s future. By implementing

GrandCare’s remote support solutions now, providers can future proof their services against budget constraints while delivering better and more independent care.
This innovative approach offers a dual advantage: significant cost savings for organizations through reduced staffing needs, while simultaneously promoting greater independence for clients. The path forward is clear, agencies that adopt these technologies today will be better positioned to:
- Maintain quality care despite funding cuts
- Reduce operational costs through automation
- Empower clients with tools for greater self-sufficiency
- Future-proof their organization against ongoing uncertainties
Now is the time to act. By investing in remote support solutions, agencies can turn the challenge of Medicaid cuts into an opportunity to deliver more sustainable, empowering care. The result? Happier, more independent clients and more financially stable organizations; regardless of what happens with Medicaid funding. The future of care isn’t about doing less, it’s about working smarter. GrandCare can provide the tools to make that future possible.


 The Leading Forum on Recovery Audits, Readmissions, Value-Based Purchasing, HACs and Never Events, and Managing to Medicare Margins
The Leading Forum on Recovery Audits, Readmissions, Value-Based Purchasing, HACs and Never Events, and Managing to Medicare Margins